Human Performance & Limitations · Module D — Poisons & The CabinSmoking & Alcohol
Chapter 9 — Two self-inflicted hazards the exam loves: the smoker's altitude penalty and oxygen-capacity loss, and alcohol — the 24-hour bottle-to-throttle rule, the fixed metabolic rate, and why altitude doubles every drink.
Plate 9.0 — Two habits, one cost: both quietly steal the oxygen and judgment a pilot cannot spare.
§ 13Smoking
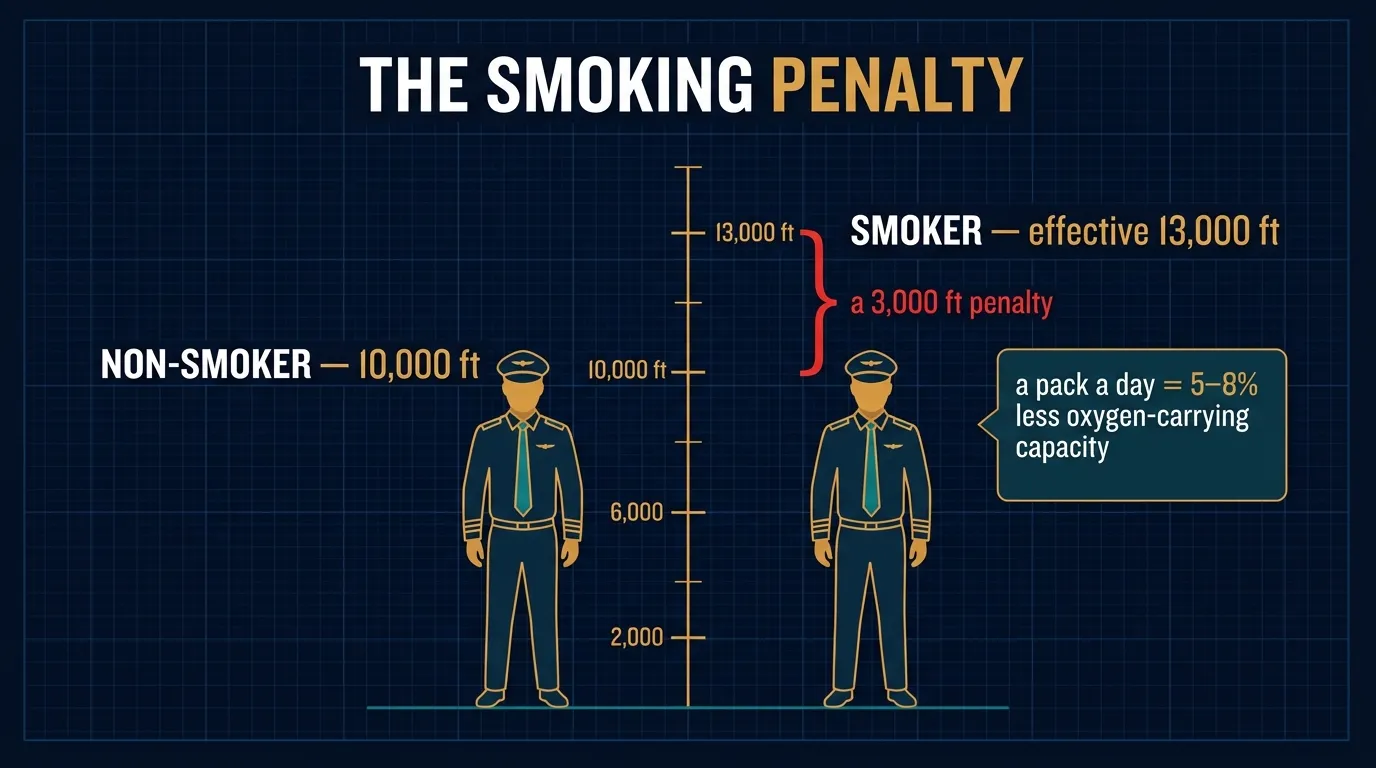
13.1 The 3,000-ft Penalty — 10,000 ft becomes 7,000 ft
The single most-asked DGCA fact about smoking
A pilot who is also a smoker may experience the symptoms of oxygen deprivation, or hypoxia, at a lower altitude (7,000 ft) than a non-smoker (10,000 ft).
That is a 3,000-ft penalty. The smoker walks into the cockpit already partway up the hypoxia ladder. Combine that with an unpressurised climb to FL080 and the smoker can be hypoxic at cruise altitude when the non-smoker beside him is still asleep.
7,000ftSmoker's effective hypoxia threshold
5–8%O₂-carrying capacity reduction — 1 pack/day
↑Increased susceptibility to CO poisoning
13.2 The 5–8 % O₂-Capacity Hit
Why smoking handicaps you — direct quote
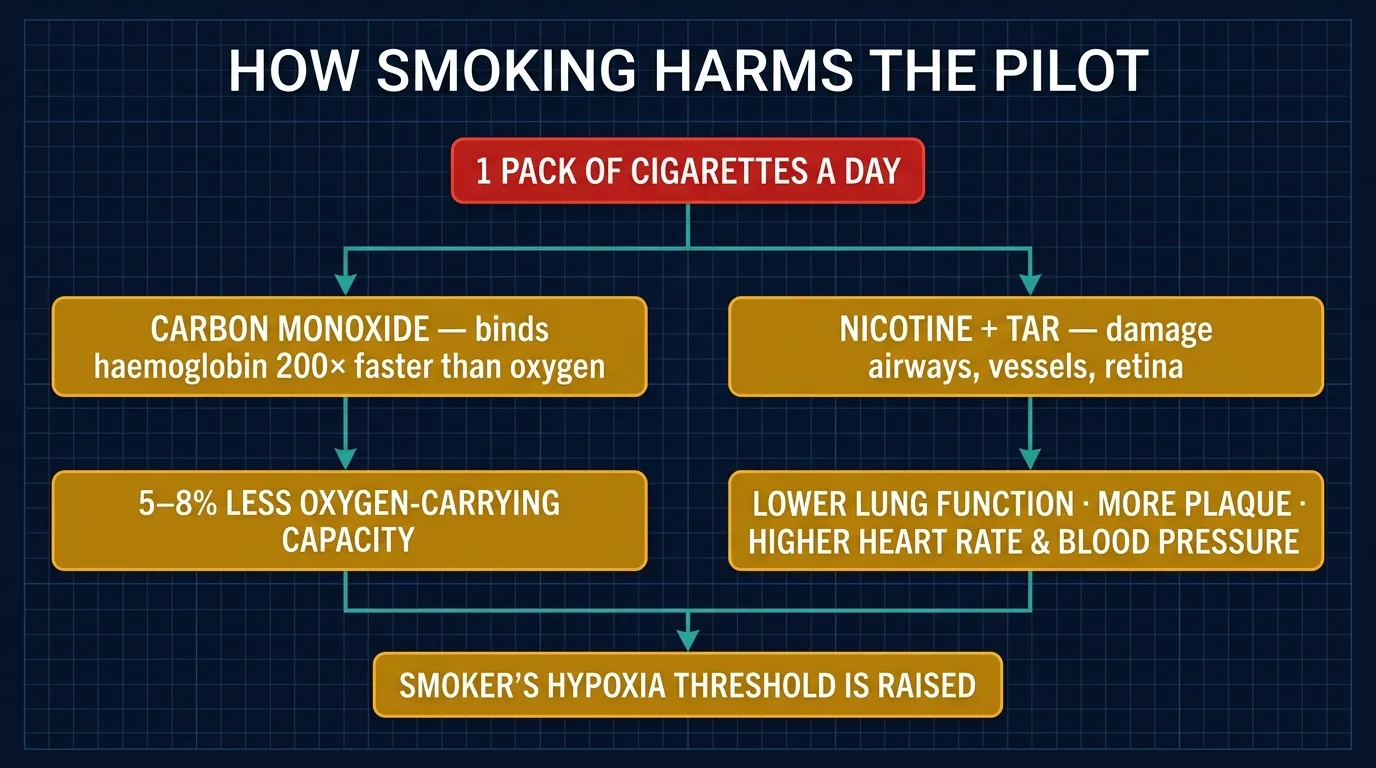
A person who smokes one packet of cigarettes per day will reduce his capacity to carry oxygen by 5–8 %. A smoker also has increased susceptibility to Carbon Monoxide poisoning.
The mechanism — anemic hypoxia, self-inflicted
Cigarette smoke contains carbon monoxide. Recall from §11.1 that CO binds to haemoglobin over 200 times more readily than oxygen. Every cigarette saturates a portion of your haemoglobin with CO — and that Hb is then unavailable to carry oxygen until the body slowly clears it (hours). A heavy smoker effectively walks around with permanent low-grade anemic hypoxia (Type b). This is why the smoker's hypoxia threshold drops 3,000 ft.
Figure 9.1 — The smoking penalty: a pack a day permanently shaves 5–8% off effective oxygen-carrying capacity, so 10,000 ft feels like 7,000 ft worse.
13.3 The Full Medical-Impact List
DGCA-quoted health effects on a smoking pilot
The smoker pilot is exposed to all six of the following — every one with direct flight-safety implications:
Lung cancer
Breathing problems
Circulatory problems
Reduced tolerance to G forces
Increased risk of heart attack
Degradation of night vision
Smoking — what it breaks and why it matters in the cockpit
Health Effect
Flight-Safety Implication
Lung cancer
Eventual respiratory failure — medical disqualification.
Critical in aerobatics, fighter pilots, upset recovery. Less G-tolerance → earlier G-LOC.
Increased risk of heart attack
Direct link to angina/MI risk-factor list in §9.5 (smoking was one of the 12 listed).
Degradation of night vision
Recall night vision is impaired at 5,000 ft for non-smokers (§10.5). Smokers see degradation at even lower altitudes — devastating for night IFR and night VFR ops.
Figure 9.2 — What smoking breaks: carbon monoxide load, reduced oxygen capacity, and the cardiovascular toll.
Practical CRM note
DGCA Class-1 / Class-2 medicals do not automatically disqualify a smoker, but the lifestyle is flagged. If you smoke and you are reading this, you are accepting a permanent flight-performance handicap. Even one cigarette before takeoff materially lowers your hypoxia threshold for that sortie. Best practice for examined fitness: do not smoke at all, especially in the 24 hours before flight.
§ 14Alcohol
The headline — alcohol is a depressantAlcohol acts primarily as a depressant. Do not fly while under the influence of alcohol. Even small amounts of alcohol in the system can adversely affect judgment and decision-making abilities.
14.1 The 24-Hour Bottle-to-Throttle Rule
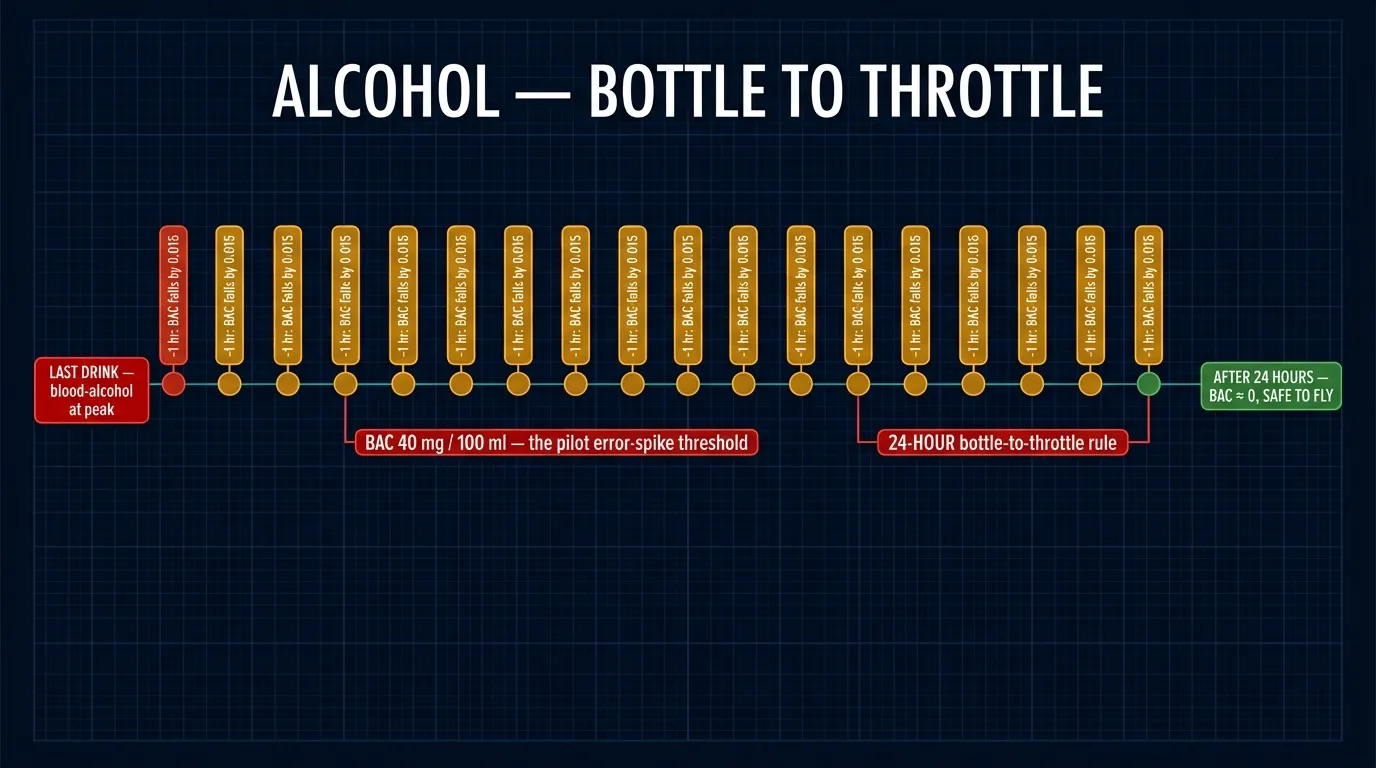
The hard rule — memorise verbatimAn excellent rule is to allow TWENTY-FOUR HOURS between the last drink and takeoff time.
This is the "24-hour bottle-to-throttle" rule. It is more conservative than the statutory minimum in some jurisdictions (often 8 hours), and is the answer DGCA expects in the HPL paper. Some operators enforce 12 hours; some, 24. The / DGCA text recommends 24 hours.
14.2 Alcohol Metabolism — The Fixed Rate
DGCA-quoted metabolism rate
Remember that your body metabolises alcohol at a fixed rate, and no amount of coffee or medication will alter this rate. Alcohol leaves the body at an average rate of 0.015 g/100 mL/hour, which is the same as reducing your Blood Alcohol Content (BAC) level by 0.015 per hour.
For men, this is usually a rate of about ONE STANDARD DRINK PER HOUR.
24hrBottle-to-throttle separation
0.015g/100 mL/hr metabolism rate (≈ 1 drink/hr in men)
40mg%BAC at which pilot errors spike significantly
14.3 Altitude Amplifies the Effect — "1 = 2" Rule
The "one drink at altitude equals two at sea level" rule
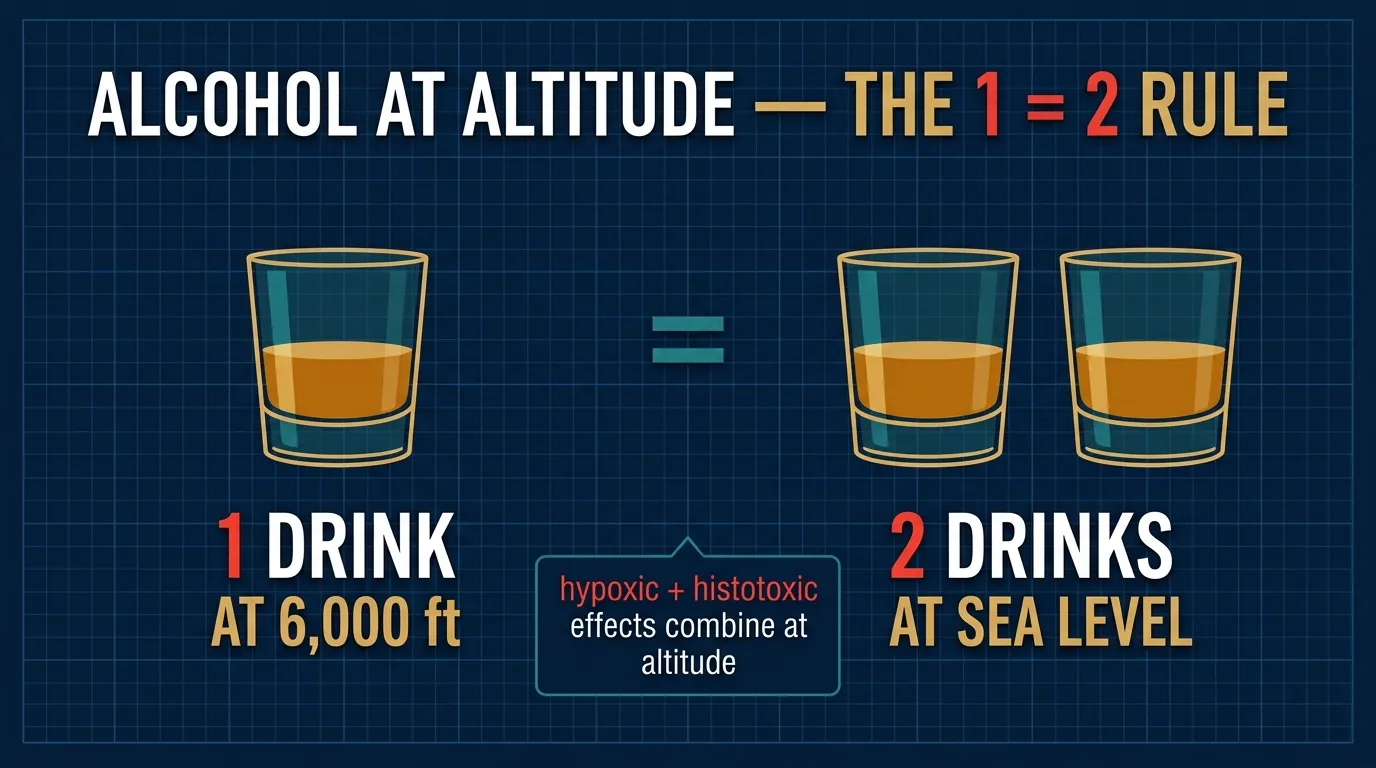
Relatively small amounts of alcohol significantly decrease a pilot's tolerance to hypoxia (oxygen lack). At 6,000 ft (1,800 m), the effect of ONE drink is that of TWO drinks at sea level. Even at sea level alcohol impairs judgment and reaction time. Therefore, alcohol and flying do not mix.
Why? — histotoxic + hypoxic stacking
Recall Histotoxic Hypoxia (§10.3d): high blood alcohol levels prevent cells from using the oxygen they receive. Layer that on top of Hypoxic Hypoxia (§10.3a) from altitude, and you have two oxygen-starvation mechanisms operating at the same time. They are additive — exactly the same principle that makes a smoker's hypoxia worse at altitude.
Figure 9.3 — The 1=2 rule: one drink at 6,000 ft hits the pilot like two at sea level (hypoxic + histotoxic effects combine).
14.4 Recommended Maximum Alcohol Intake — Units & Rules
Definition of "one unit"ONE UNIT of alcohol = half a pint of beer = a standard glass of wine = one measure of spirits.
MEN
5 units / day · 21 units / week
Maximum recommended consumption.
WOMEN
3 units / day · 14 units / week
Maximum recommended consumption.
1 unit equals
½ pint beer
1 unit equals
1 glass wine
1 unit equals
1 measure spirits
Men – daily/weekly
5 / 21
Women – daily/weekly
3 / 14
14.5 BAC 40 mg/100 ml — The Pilot Error-Spike Threshold
DGCA-quoted: the BAC level at which errors balloonBlood alcohol concentrations of 40 mgs per 100 ml results in significant increases in errors committed by pilots due to the following effects:
Impaired judgment and impaired ability to reason
Degraded muscular coordination and degraded vision
Lack of inhibitions and self-control
Increased susceptibility to Hypoxia
Damages to the liver, heart, brain and blood cells
Affects short and long-term memory
Slows reaction time
Sufferer may feel that performance is improved(the alcohol-euphoria trap)
Balance and sensory illusions
Irregular sleep patterns
The euphoria trap — analogous to hypoxia
"Sufferer may feel that performance is improved" is the alcohol equivalent of hypoxia's euphoria (§10.2). The pilot is the least qualified person in the cockpit to judge whether he's safe to fly. This is precisely why fixed bottle-to-throttle rules exist — they take the judgement out of the impaired pilot's hands.
14.6 Hangover & the "Masked Hangover" Warning
DGCA-quoted hangover rule — verbatimDo not fly with a hangover, or a "masked hangover" (symptoms suppressed by aspirin, caffeine or other medication). High altitude, where oxygen is deficient, aggravates these effects.
Why a "masked" hangover is worse than an obvious one
A normal hangover at least gives you a warning sign — you feel awful, you don't fly. A masked hangover, where caffeine, paracetamol, ibuprofen or other OTC medication has suppressed the headache and nausea, leaves you still impaired in judgement, coordination, vision and reaction time — but without the warning. Several aviation accidents have been traced to a pilot who took an aspirin, "felt fine," and flew with substantial residual BAC.