Human Performance & Limitations · Module D — Poisons & The CabinThe Cabin Environment
Chapter 10 — The physical environment around the pilot: humidity, temperature, vibration, glare and UV, and what happens when a pilot is incapacitated in flight — from a simple faint to a fit.
Plate 10.0 — The pilot's physical world: the heat, glare, dryness and vibration that quietly wear performance down.
§ 23Humidity
23.1 Why Humidity Matters Up High
DGCA-quotedHumidity may become an issue with high-altitude jet transport aircraft because of the low relative humidity at their operational altitudes. The discomfort arising from low relative humidity may not imply physical indisposition.
DGCA-quoted humidity ranges
40 – 60 % relative humidity is NORMAL.
< 20 % may create minor discomfort, such as skin, eye, nose, throat dryness.
3–8% → 22%Modern humidifiers raise cabin RH from 3–8% to ~22%
Prevention & management
Overall dehydration can be prevented with adequate fluid intake.
Diuretics like coffee or tea should be avoided. They drive fluid out of the body via increased urination — the opposite of what is needed at altitude.
23.2 Aircraft Humidifier Systems
DGCA-quoted
The installation of humidifiers on aircraft raises cabin/cockpit humidity, but there are potential problems such as:
Weight penalty,
Condensation, and
Mineral contamination that the designer must consider.
Aircraft such as the Airbus A350, Boeing 787, and the future Boeing 777X are compatible with onboard humidifiers, either in crew areas or the entire cabin. These technologies increase humidity from 3–8 % to 22 % and reduce contaminants in the air we breathe on a flight.
§ 24Temperature
DGCA-quotedTemperature affects performance as follows:
24.1 The Three Reference Temperatures — memorise verbatim
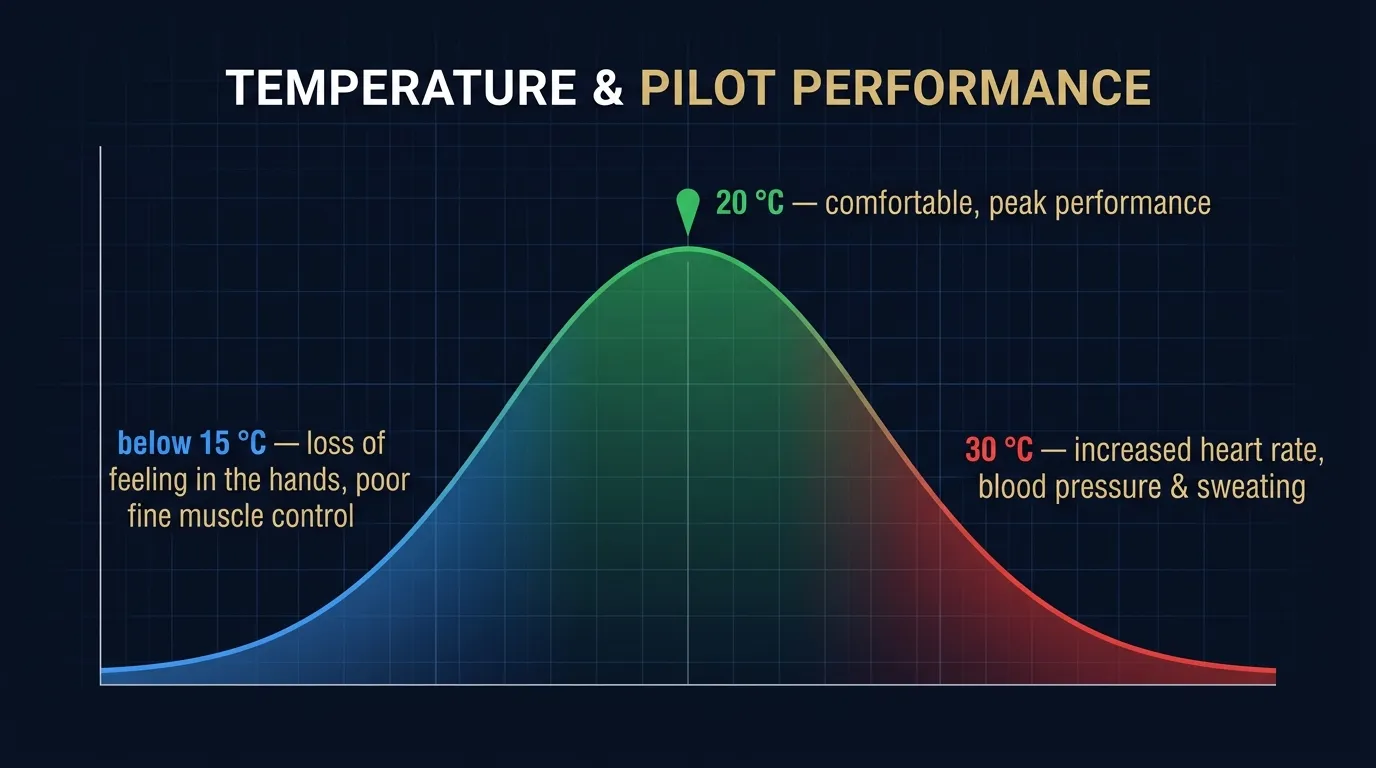
Temperature effects on pilot performance (DGCA verbatim)
Temperature
Effect on Performance
20 °C
Comfortable temperature for most people in normal clothing.
30 °C
Increased heart rate, blood pressure, and sweating.
> 15 °C
Discomfort, loss of feeling in hands, poor control of fine muscle movement.(Note: source phrasing uses "> 15 °C" — referring to deviations beyond 15 °C from a comfortable baseline, i.e. cold-stress.)
Cockpit-temperature considerations
At 20 °C the pilot is comfortable — fine motor skills, judgement and reaction time are optimal.
At 30 °C the body's ANS responds to heat stress by raising HR, BP and triggering sweating to cool the skin. Cognitive performance starts to degrade.
In cold conditions — far below the comfort baseline — the pilot loses sensation in the fingers, struggles with fine-motor tasks like switch selection or fast checklist scanning, and may shiver involuntarily.
For both extremes, cabin temperature management is a flight-safety task, not merely a comfort one. Climate control should be set to keep cockpit temperature near 20 °C for sustained operations.
Figure 10.1 — Pilot performance peaks around 20 °C; both cold and heat degrade it in their own way.
§ 25Vibration
25.1 Natural Resonance — Why Frequency Matters
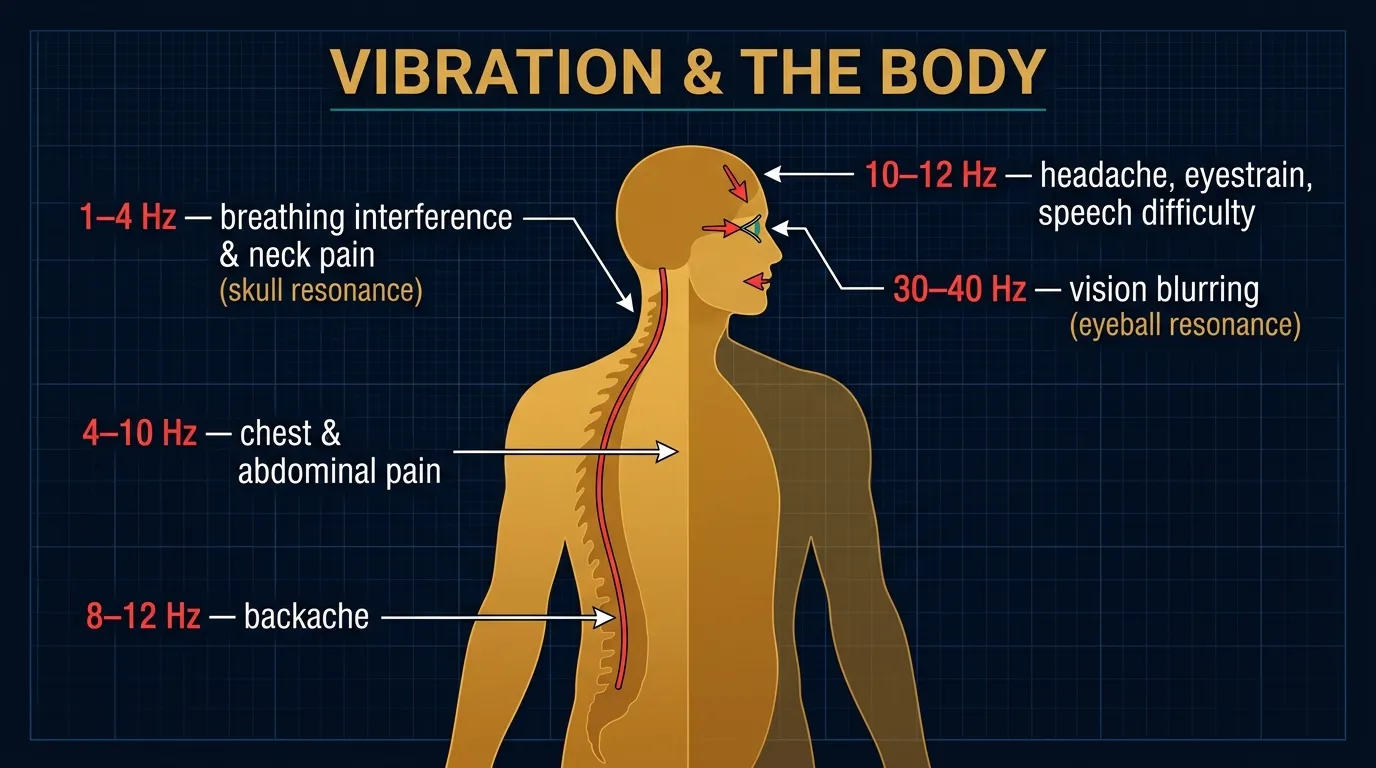
DGCA-quoted openingDifferent parts of the body show a natural resonance at different periods of vibration. For example:
The natural resonance of the eyeball is 30 – 40 Hz, and
The skull is 1 – 4 Hz.
What "natural resonance" means in plain English
Every physical structure has a frequency at which it wants to vibrate — push it at that frequency and small inputs build up into huge oscillations (think of pushing a child on a swing in time with the swing's natural period). When external aircraft vibration matches a body part's resonant frequency, that part suffers maximum disturbance. The eyeball resonating at 30–40 Hz is precisely why vision becomes blurred at certain helicopter or propeller-vibration frequencies.
25.2 Effects of Vibration — Full DGCA Frequency Table
Memorise this table — direct exam target
Effects of vibration include:
Vibration frequency vs body effect (DGCA verbatim)
Frequency Range
Effect on the Body
1 – 4 Hz
Interference with breathing; neck pain.(Skull resonance range.)
This is why aircraft seats incorporate damping and isolation systems — to keep the airframe's vibration spectrum from delivering energy at the worst body-resonance frequencies.
§ 26Glare & UV Radiation
DGCA-quotedUV radiation from sunlight can cause visual fatigue, as well as affect visual health.
Why glare and UV deserve their own section
At cruise altitudes (FL300+), the protective filtering of the atmosphere is reduced. Cockpit windows admit significantly more UV-A and UV-B than ground-level glass would. Over a long career, this contributes to:
Visual fatigue — the immediate effect of glare on the working pilot. Squinting, eyestrain, reduced contrast sensitivity, headache.
Use aviation-grade polarised or non-polarised UV-blocking sunglasses (note: certain LCD instruments may distort under polarised lenses — check before adoption).
Use cockpit sun-visors appropriately — don't leave them stowed when the sun is over the nose.
For long-haul crews, schedule vision rest breaks on autopilot legs.
Periodic aero-medical eye examinations — already mandated by DGCA — pick up early cataract / retinal changes.
§ 27INCAPACITATION IN FLIGHT
27.1 Why Pilot Incapacitation is a Flight-Safety Issue
DGCA-quoted introduction — verbatimThe risk of seizure in flight is obvious. Incapacitation is in most cases:
Sudden,
Unpredictable,
Unavoidable,
Prolonged,
Complete, and
Potentially more frequent in the stressful flying environment,
… and constitutes a direct threat to the health and safety.
DGCA-quoted prevention measurePeriodical medical examinations minimize the risk of incapacitation in flight. The frequency of medical checks increases with advancing age.
Class-1 medical (commercial pilot) under 40
12 months
Class-1 medical, 40+
6 months
Class-2 medical (PPL) under 40
5 years (varies)
Class-2 medical, 40+
2 years (varies)
(The DGCA medical-frequency periods are referenced in the syllabus generally and shown above for context; exact CAR / Schedule periods should be confirmed against the latest DGCA medical CAR / FAA Part 67 equivalent.)
27.2 Obvious Incapacitation
DGCA-quoted definitionObvious incapacitation normally refers to a state in which all of a crew member's physical or mental functions are lost, including:
Loss of consciousness, OR
Being unable to move while retaining consciousness,
… rendering them completely unable to carry out their duties.
Onset patterns & presentation
Obvious incapacitation can sometimes involve convulsions,
OR the victim may lapse into unconsciousness several minutes after the incapacitation occurs.
Interracial hemorrhage(intended: "intracranial haemorrhage" — bleed in the brain)
Cerebral apoplexy(stroke)
Epilepsy
The source PDF uses the phrasings shown — students should be aware of the modern medical terminology in parentheses.
27.3 Subtle / Insidious Incapacitation
DGCA-quoted definitionSUBTLE (develops slowly and gradually), incapacitation refers to a state of a partial or temporary loss of physical or mental function which manifests itself in the form of:
Partial paralysis,
A dulling of perception, judgment, or responses or lack thereof,
A state of absence of mind, distraction of attention,
Trouble with speech,
Inadequate responses,
Meaningless utterances, etc.
The hidden-danger warning — DGCA verbatimParticular attention must be paid to the fact that a crew member may become incapacitated EVEN THOUGH THEIR APPEARANCE IS NO DIFFERENT FROM NORMAL.
Possible causes of subtle incapacitation — DGCA list
Temporary hypoglycemia (low blood sugar — pilot skipped meals)
Reduction in blood pressure
Cerebropathy or psychopathy
Excessive muscular fatigue
Excessive drinking (see §14)
Insufficient sleep
Emotional instability
Toothache
Stomachache
Headache
27.4 Obvious vs Subtle — Why Subtle is MORE Dangerous
DGCA-quoted — the counterintuitive truthSince other crew members are often unable to detect subtle incapacitation quickly, from a flight safety point of view, it is possible that SUBTLE INCAPACITATION MAY LEAD TO A SITUATION OF COMPARATIVELY GREATER DANGER THAN OBVIOUS INCAPACITATION.
Why this matters in two-crew operations
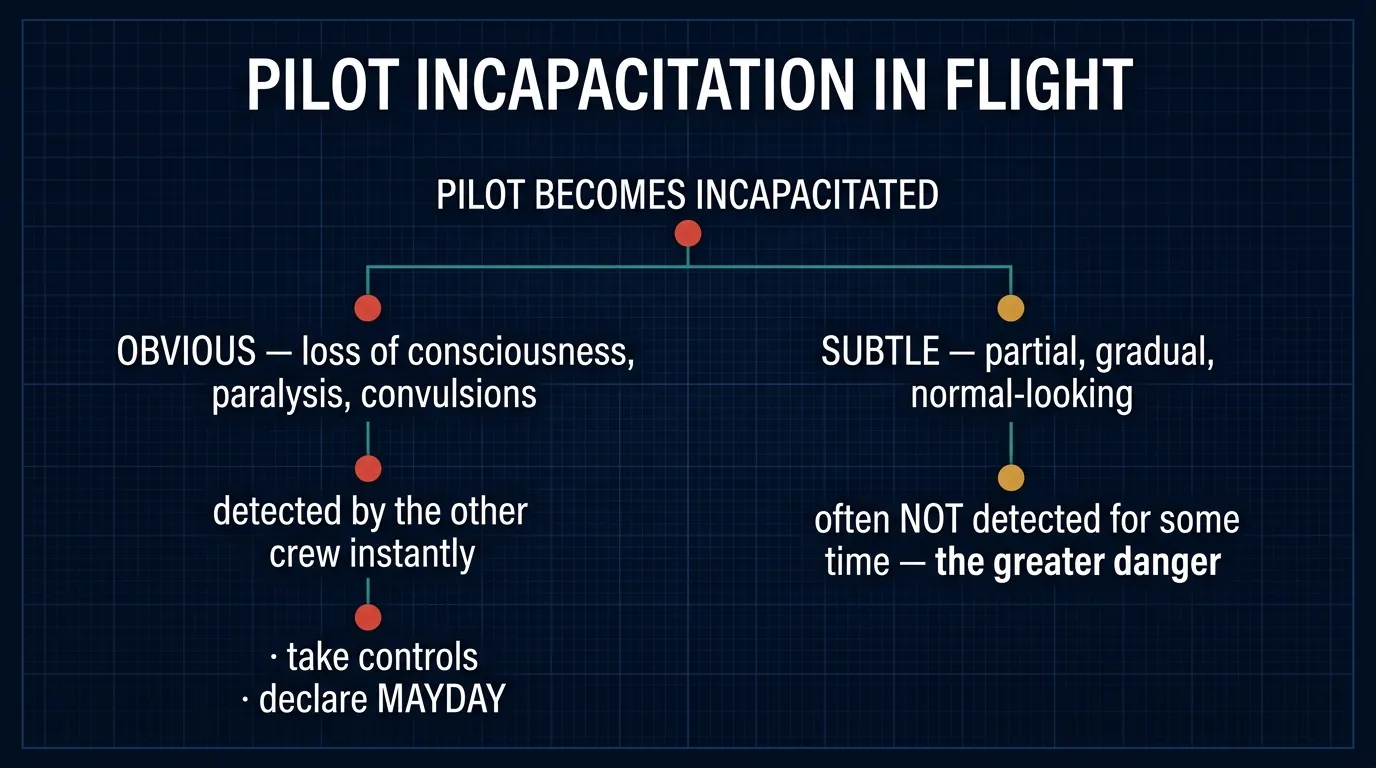
With obvious incapacitation, the other crew member sees the captain slumped or convulsing, declares emergency, takes control, gets the aircraft on the ground. The hand-off is instant.
With subtle incapacitation, the captain is still moving switches, talking on the radio, even responding to questions — but his judgement is impaired. He may set the wrong altitude, mis-tune a NAV, mishear an ATC clearance, or fail to initiate a missed approach. The other pilot may not detect this until after the wrong outcome unfolds. This is the rationale behind two-crew CRM: a healthy independent cross-check that catches subtle drift before it becomes an accident.
Figure 10.3 — Pilot incapacitation: recognising it and the other crew member's response.
§ 28FITS & FAINTS
28.1 Epilepsy — Grand Mal & Petit Mal
DGCA-quoted definition
A fit or seizure is usually referred to as "epilepsy". A fit or a seizure is not a specific disease but a set of signs or symptoms in response to a disturbance of the electrical activity in the brain.
Grand Mal Epilepsy
Manifests as a generalized seizure
Associated with a transient loss of consciousness
May be associated with a prodromal phase(warning aura before the seizure)
Normally accompanied by convulsions and uncontrolled physical movement
Petit Mal Epilepsy
Also a generalized seizure
Not associated with a loss of consciousness
Petit Mals are a MINOR attack
Often presents as brief "absence spells" — staring, blanking out for a few seconds
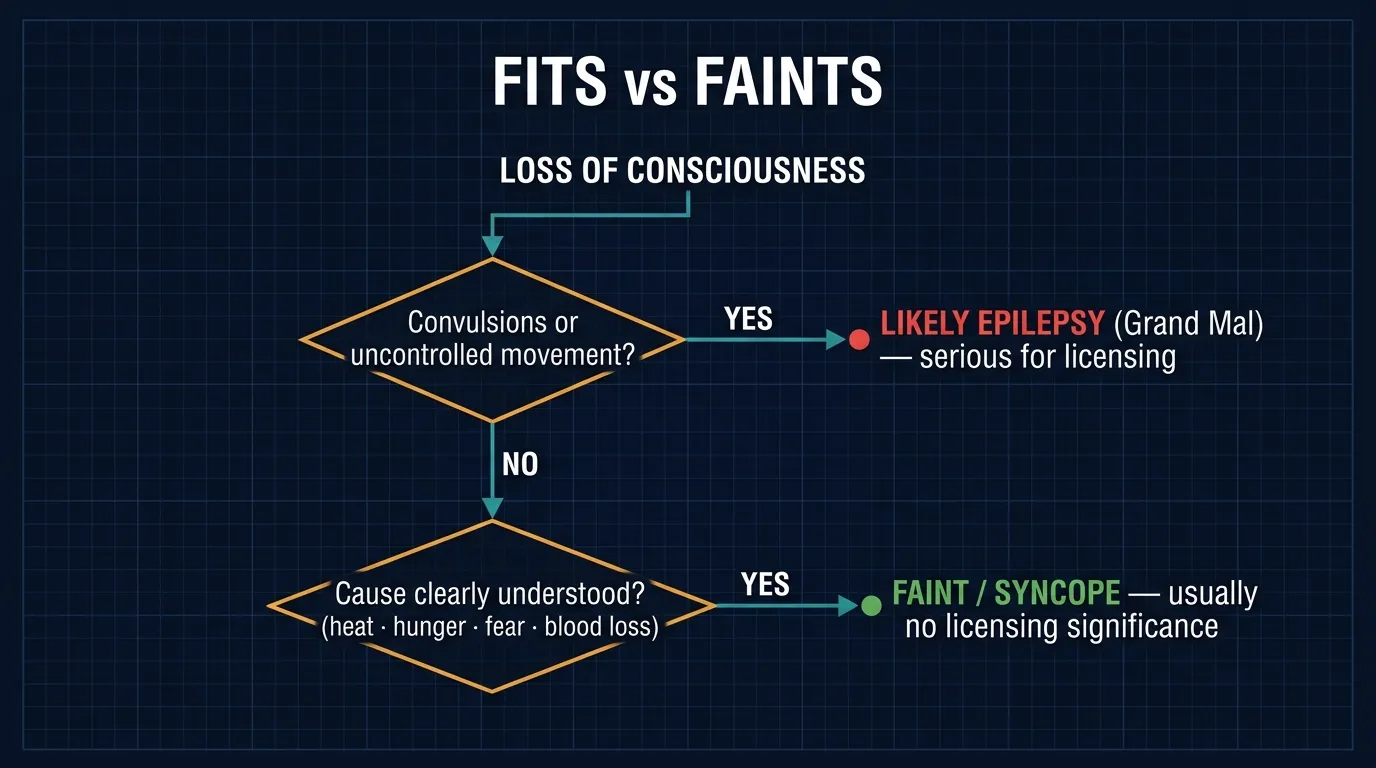
DGCA-quoted — the absolute barA seizure may or may not be associated with a loss of consciousness… but ANY FIT, MAJOR OR MINOR, IS ASSOCIATED WITH AN UNPREDICTABLE LOSS OF CONSCIOUSNESS AND IS THEREFORE AN ABSOLUTE BAR TO THE HOLDING OF A FLYING LICENCE.
Pilot-medical implication
This is one of the very few absolute medical disqualifications in aviation. Even controlled epilepsy on medication — even a single documented seizure event in adult life — is grounds for medical refusal. The reason is the word "unpredictable" — DGCA cannot certify the probability of an in-flight seizure as acceptably low.
28.2 Faint & Vasovagal Syncope
DGCA-quoted definitionFaint is a common cause of a loss of consciousness in adults. The most common causes of faints are:
Common causes of faint — DGCA verbatim list
#
Cause
1
Standing up quickly after prolonged sitting especially when hot or dehydrated
2
A sudden shock
3
Loss of blood after an accident
4
Lack of food or fluid
5
Other physiological stress
DGCA-quoted — Syncope & Vasovagal SyncopeSyncope is a temporary but sudden loss of consciousness when blood flow to the brain is compromised. In young individuals, fear, anxiety, sight of blood, etc., can result in a temporary loss of consciousness. This is referred to as VASOVAGAL SYNCOPE.
Frequently, syncope is associated with symptoms like:
Light-headedness,
Muscle weakness, and
Dizziness before the actual fainting occurs.
DGCA-quoted — flight-licence implicationA faint has NO SIGNIFICANCE as far as future flying is concerned, so long as the cause is clearly understood.
Epilepsy vs Faint — the critical comparison
This is the most frequently tested contrast in DGCA HPL papers. Memorise it:
Epilepsy vs Faint (Syncope) — side-by-side
Parameter
Epilepsy (Grand/Petit Mal)
Faint (Syncope)
Underlying cause
Disturbance of brain electrical activity
Compromised blood flow to the brain
Loss of consciousness
Often (Grand Mal) / Absent (Petit Mal)
Yes, temporary & sudden
Convulsions / uncontrolled movement
Yes (Grand Mal)
No
Predictability
Unpredictable
Cause is usually identifiable (heat, hunger, fear, blood loss)