Human Performance & Limitations · Module C — The Thin AirPressure, TUC & Decompression
Chapter 8 — What happens when the pressure fails: cabin pressurisation and the shrinking Time of Useful Consciousness, decompression, the bends, and the rules for blood donation and flying after diving.
Plate 8.0 — When the pressure fails. At altitude the margin between control and unconsciousness is measured in seconds.
§ 16Baroreceptor Reflex
What it is
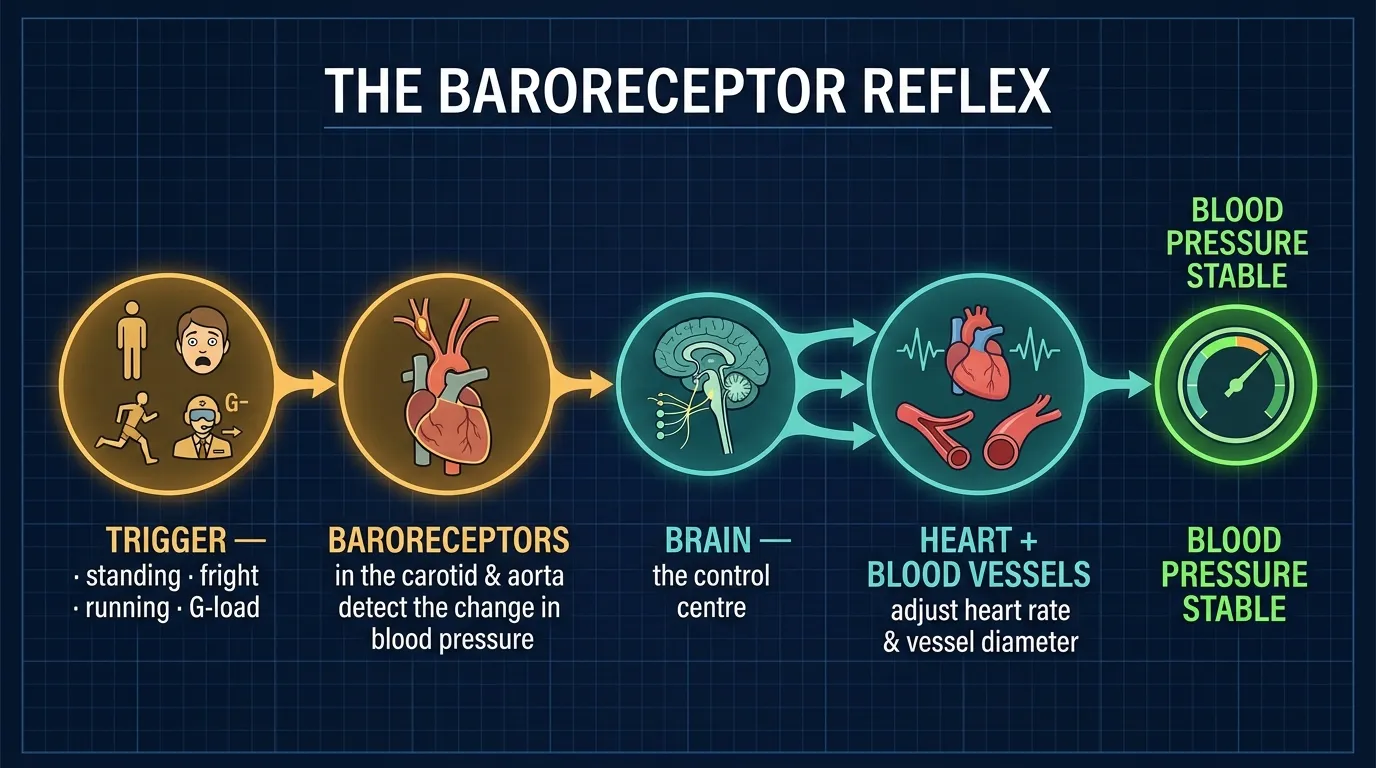
The baroreceptor reflex is the body's automatic blood-pressure regulator. Any change in your body's demand for blood can trigger your baroreceptor reflex. Specialised pressure-sensors ("baroreceptors") in the carotid arteries and aortic arch detect changes in BP and signal the brain to adjust heart rate and vessel diameter accordingly.
16.1 When the reflex fires — DGCA examples
For example, your body may need to adjust your blood pressure when you:
Change your body position, such as when you stand.
See or experience something that frightens you.
Switch from walking to running.
Cockpit relevance
Postural changes: standing up from a long sit (e.g. after a long flight, in turbulence, or after a low-blood-sugar moment) can cause transient hypotension → light-headedness. The baroreceptor reflex normally corrects this in 1–2 seconds.
Sudden fright / startle response: pulls in adrenaline from the ANS (§7.4), spiking HR and BP. The baroreceptor reflex moderates this so you don't pass out from a hypertensive crisis.
Exercise & G-load: from steady cruise to sudden manoeuvring, blood demand changes rapidly. The reflex keeps cerebral perfusion stable so you don't grey out.
A well-conditioned, well-rested, well-hydrated pilot has a sharper, faster baroreceptor reflex. A dehydrated or fatigued pilot's reflex is sluggish — which is one of several reasons hydration matters in long sectors and high-G ops.
Figure 8.1 — The baroreceptor reflex: how the body senses and corrects a fall in blood pressure.
§ 17Donating Blood — the 48-hr rule
DGCA-quoted
In a completely healthy individual, the fluid reduction caused by donating one unit of blood is replaced within several hours. In some people, however, the loss of blood causes disturbances to the circulation that may last for several days.
While the effects at ground level are minimal, flying during this period may entail a risk.
The DGCA rule — exact phrasingGenerally, active pilots should NOT donate blood, but if blood has been donated, they should wait at LEAST 48 hours before flying.
Recommended for active pilots
DO NOT donate
If donation has occurred
Wait ≥ 48 hr
Reason
Circulatory disturbance
Ground-level effect
Minimal
Why blood donation interacts dangerously with flight
A single unit of blood (~450 ml) represents about 9 % of total blood volume in an average adult. While the plasma volume is restored in hours, the red blood cell mass takes weeks to fully recover. Reduced RBC mass = reduced haemoglobin = reduced oxygen-carrying capacity = anemic hypoxia (§10.3b). Add altitude (hypoxic hypoxia, §10.3a) and the two stack — exactly the same principle as smoker-at-altitude and alcohol-at-altitude in Part 4.
§ 18Cabin Pressurization & Time of Useful Consciousness (TUC)
18.1 What TUC / EPT is
Definition — memorise verbatimTime of useful consciousness (TUC), also effective performance time (EPT), is defined as the amount of time an individual is able to function effectively (e.g., perform flying duties) in an environment of inadequate oxygen supply.
It is the period of time from the interruption of the oxygen supply or exposure to an oxygen-poor environment to the time when useful function is lost, and the individual is no longer capable of taking proper corrective and protective action.
Critical concept — TUC is NOT time to unconsciousness
TUC is the time during which a pilot can still do useful work — don a mask, push a checklist, initiate descent. After TUC ends, the pilot may still be conscious for several more seconds, but is no longer functional. This distinction is precisely why the DGCA emphasises "corrective and protective action" — the mask must be on the face before TUC expires.
18.2 Why TUC Drops Sharply at Altitude
DGCA-quoted
At the higher altitudes, the TUC becomes very short; considering this danger, the emphasis is on PREVENTION rather than CURE.
Cabin pressurization eliminates many problems associated with high altitude flying, but it introduces other potential problems, the most important being the risk of rapid decompression.
What determines TUC after a rapid decompression
The time of useful consciousness (TUC) following a rapid decompression depends on:
Aircraft altitude,
The rate at which pressure falls, and
The level of physical activity of the individual at the time of the event.
Jet-transport TUC reference values
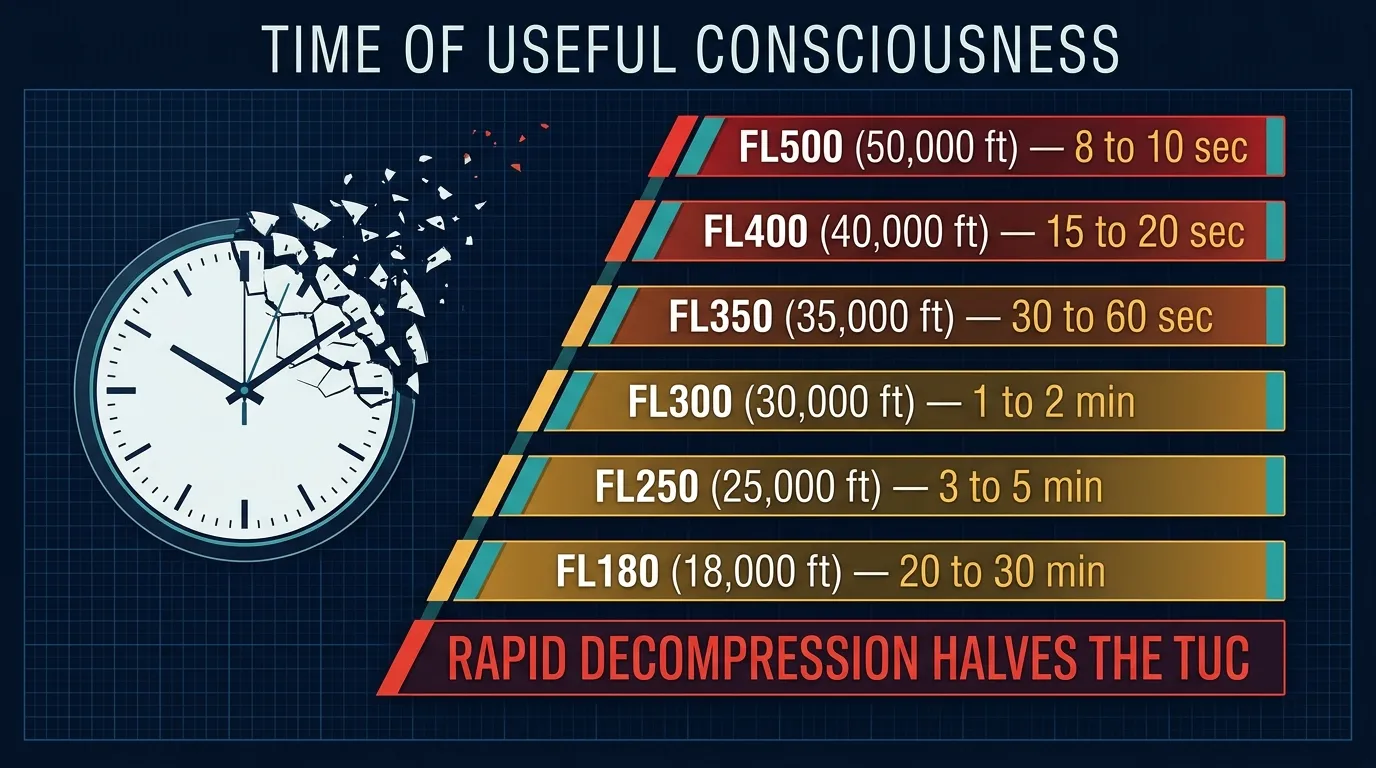
At typical jet transport aircraft altitudes (35,000 feet) TUC will vary between 33 and 54 seconds.
Those average values can be expected to drop by HALF at 40,000 feet.
This emphasizes the importance of immediate availability of supplemental oxygen to crew members.
RAPID DECOMPRESSION CAN REDUCE TUC BY HALF.
18.3 TUC Master Table — Verbatim
This is the table you must memorise — both columns. Every DGCA HPL question on TUC is drawn from these figures.
Time of Useful Consciousness (TUC) by Altitude — DGCA Reference
Figure 8.2 — Time of Useful Consciousness collapses with altitude: above FL250 it falls fast; by FL400 it is under 20 seconds.
18.4 Rapid Decompression Halves TUC
The "halving rule" — DGCA-quoted"Rapid decompression can reduce TUC by half."
Why? Because a rapid decompression doesn't just drop the pilot to ambient pressure — it actually sucks oxygen out of the lungs into the cabin atmosphere (Henry's law, in reverse). The pilot is left with less oxygen in the bloodstream than the new ambient pressure alone would predict.
33–54sTUC at FL350 (normal ascent)
½Reduction after rapid decompression
7–10sTUC at FL400 (rapid decompression)
Operational pilot response — the drill
After a rapid decompression in a transport jet you have seconds, not minutes:
Don oxygen masks immediately — quick-don, regulator to EMERGENCY/100 %.
Establish crew communication.
Initiate emergency descent — target 10,000 ft or MSA, whichever higher.
Squawk 7700, declare MAYDAY.
This drill is muscle-memory in transport flight training precisely because there is no time to think it through at FL350+.
§ 19Decompression — Theory
Definition"Decompression" means the lowering of pressure.
19.1 The 8,000 ft "Maximum Comfort" Rule
DGCA-quotedThe maximum altitude without oxygen at which flying efficiency is not impaired is 8,000 feet.
DGCA-quoted — flight risk below 10,000 ftWhen flying at altitude below 10,000 feet, the risk of suffering from conditions related to decompression is low.
19.2 Atmospheric Pressure is Halved at 18,000 ft
Nitrogen saturation & pressure facts
At ground level, the body tissues are saturated with nitrogen, the inert gas which makes up 80 % of our atmosphere.
As the aircraft climbs, atmospheric pressure is reduced.
By 18,000 ft ASL (5,486 m) atmospheric pressure is HALVED.
Decompression sickness symptoms may develop at 18,000 ft and above.
Pilots flying aircraft with unpressurised cabins at altitudes greater than 25,000 feet ASL (7,620 m) may be subject to "the bends".
19.3 The Bends — Physiology of Nitrogen Bubbles
The bottle-of-soda mechanism — DGCA's own analogy
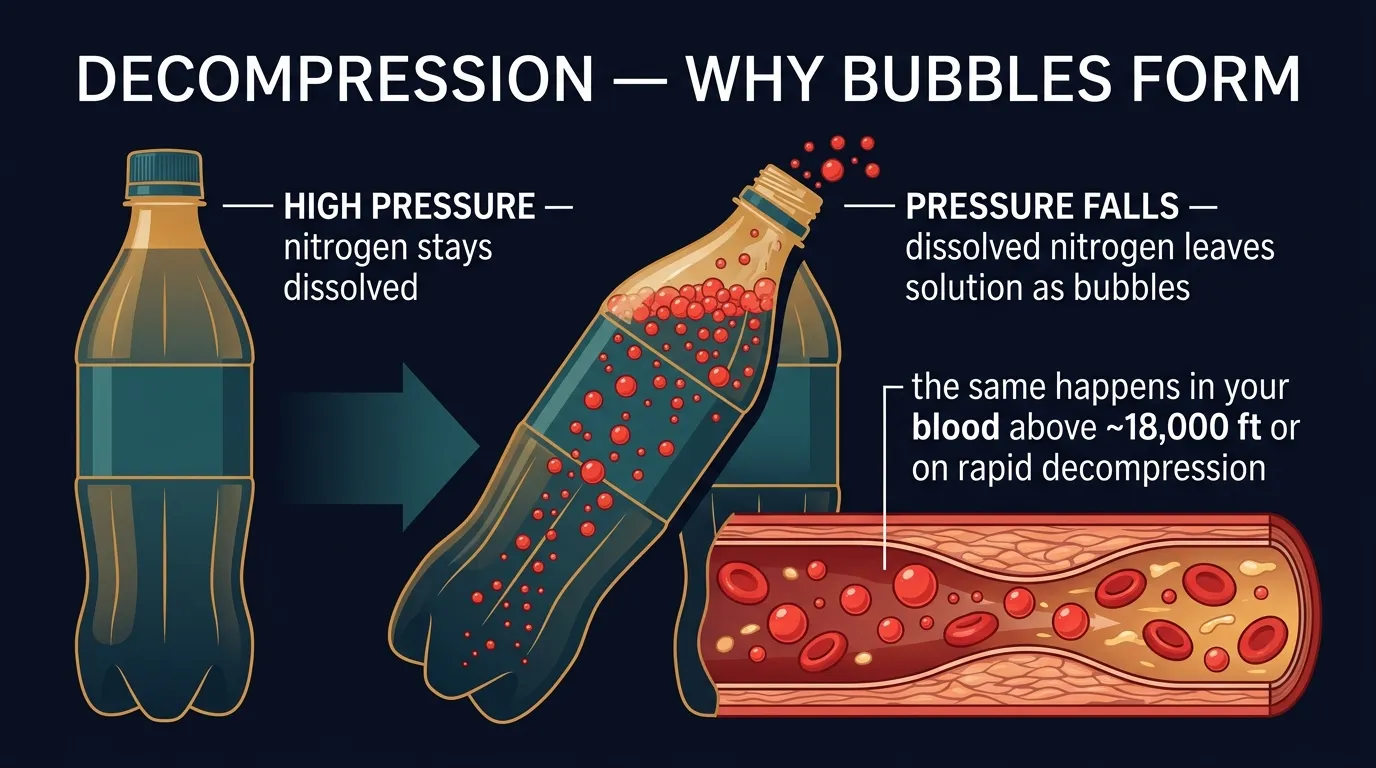
"The bends" condition is caused by bubbles of nitrogen forming in the tissues because the ambient (atmospheric) pressure is less than the pressure at ground level. (An example of this phenomenon is the bubbles formed when a bottle of soda pop is opened, and the pressure is reduced.)
The bubbles may:
Track into joint spaces causing a dull, sickening pain.
More dangerously they may be released into the lungs or the brain, giving rise to chest pain and/or collapse.
Figure 8.3 — When pressure falls, dissolved nitrogen leaves solution and forms bubbles in the blood and tissues.
19.4 Cabin Pressurization & Rapid vs Slow Decompression
How airline cabins solve the problemAirlines and high-performance aircraft have cabin pressurization systems to maintain an artificially "low altitude" within the cabin or cockpit. The pressurization of a commercial airliner flying at 30,000 ft maintains an internal cabin pressure equivalent to about 6,000 ft, with a maximum pressure of 8,000 ft.
FAST (Rapid) Decompression
A fast decompression is recognizable by:
Mist in the cabin
Blast towards the exterior of the aircraft
Expansion of body gases
Blast of air released violently from the lungs
SLOW Decompression
A slow decompression may be caused by:
A slight air-tightness defect, or
Bad functioning of the pressurization.
Insidious onset — no warning blast, no mist, but cabin altitude creeps up over minutes. Detected via the cabin-altitude warning horn (typically at ~10,000 ft cabin altitude in transport jets).
19.5 Factors that Increase the Tendency to Develop the Bends
Five DGCA-quoted predisposing factors
The tendency to develop the bends increases with:
High rates of climb,
Age,
Obesity,
Physical activity,
Low temperatures.
Max altitude without O₂ — no impairment
8,000 ft
Low DCS risk below
10,000 ft
Atmospheric pressure halved at
18,000 ft
Unpressurised flight — bends threshold
> 25,000 ft
Typical airliner cabin altitude
≈ 6,000 ft
Maximum cabin altitude
8,000 ft
N₂ % in atmosphere
≈ 80 %
DCS risk factors count
5
§ 20Decompression Sickness (DCS)
DGCA-quoted introductionWithout a cabin pressurization system, pilots and passengers in high flying aircraft would be exposed to high altitude, like hypoxia, low temperatures and Decompression Sickness/Illness.
20.1 Henry's Law Revisited — the underlying physics
Henry's Law statement — verbatim from DGCAHenry's Law explains the occurrence of decompression sickness. The principle that at a constant temperature the concentration of a gas dissolved in a fluid with which it does not combine chemically is almost directly proportional to the partial pressure of the gas at the surface of the fluid.
A rapid reduction in ambient pressure may cause the nitrogen in our blood to come out of solution as small bubbles leading to decompression sickness.
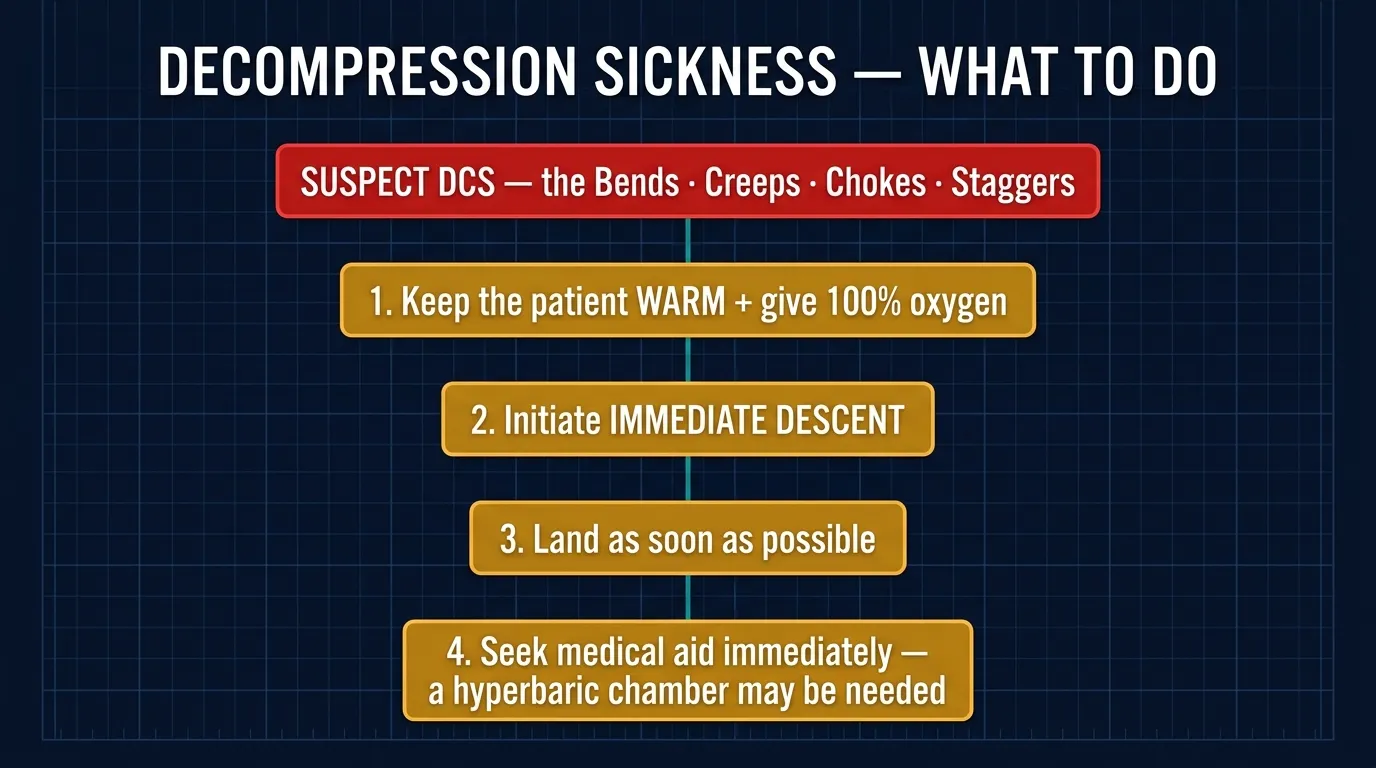
Symptom list & the "delayed onset" warningSymptoms of decompression sickness are:
Bends
Chokes
Skin manifestations
Neurological symptoms
Circulatory shock
Symptoms may appear several hours after the exposure.
20.2 Effects of Nitrogen Bubbles — Four Syndromes
The DGCA syllabus names four specific syndromes based on the tissue affected. Memorise the names and the body region.
JointsThe BENDS
Joints: Bubbles in the joints cause rheumatic-like pain, called the Bends.
Figure 8.4 — Decompression sickness (the bends): the forms it takes and the response.
20.4 The 12-Hour No-Fly Rule After Rapid Decompression
DGCA-quotedDo not fly for at least 12 hours after experiencing rapid decompression even though you may be feeling fit.
Why 12 hours?
DCS symptoms can be delayed for several hours. Feeling "fit" immediately after a decompression event does not mean nitrogen bubbles are not still forming or growing in tissues. The 12-hour pause allows the body to off-gas the residual nitrogen at normal pressure, much like a diver waiting before flying or driving up a mountain.
§ 21Flying After Diving — the 24-hour rule
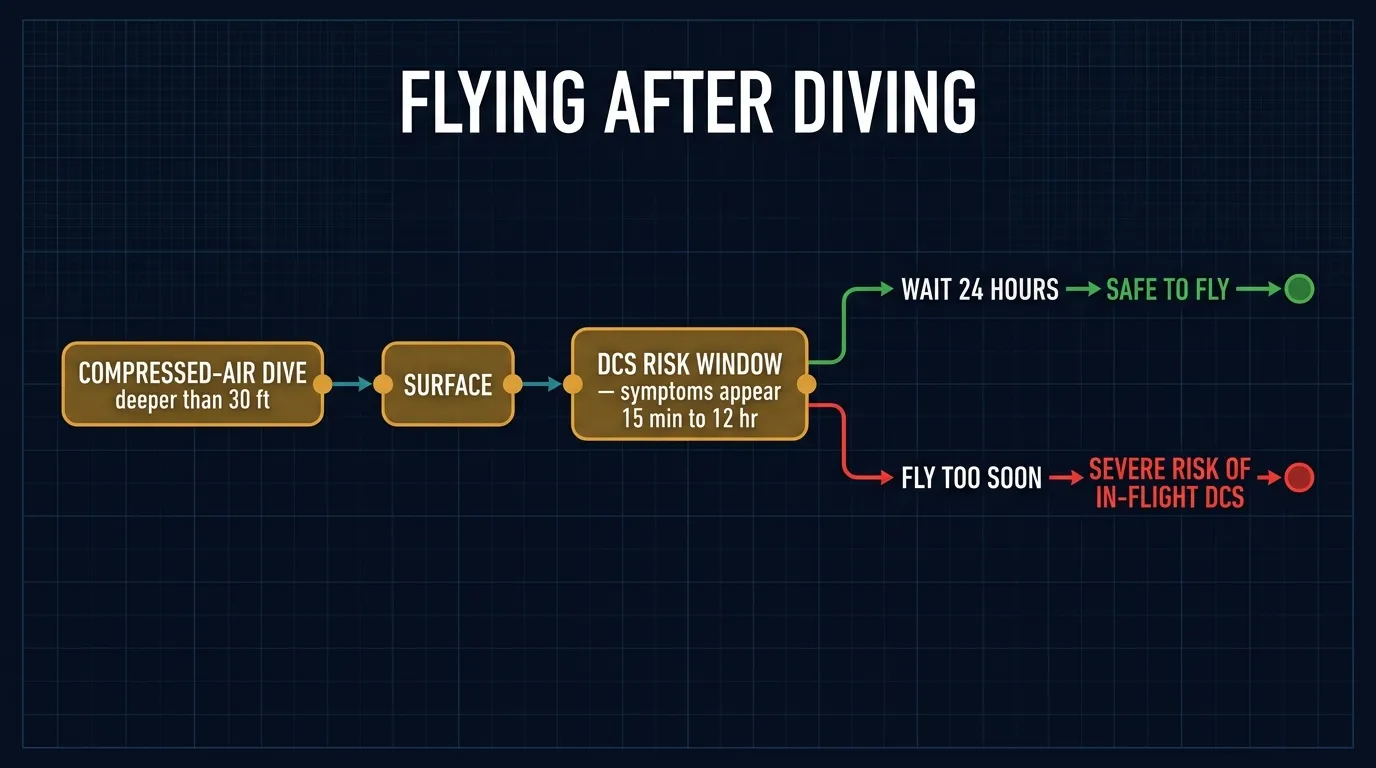
DGCA-quoted mechanismDecompression sickness can occur when flying at low altitude in individuals who have been diving, using compressed air breathing apparatus shortly before flight at a depth of 30 feet or more.
The hard rule — memorise verbatimAs a general rule, individuals should NOT fly within 24 hours following diving and certainly not the same day.
30ftDiving depth that creates DCS risk on flying
24hrMinimum wait between diving & flight
15min – 12hrSymptom-onset window after surfacing
Why diving + flight is so dangerous — DGCA-quoted
Occasionally a "medical emergency" arises as a result of compressed-air diving, when a diver is in danger of developing air-embolism (bends) at the surface altitude, as a result of being unable to decompress before surfacing. In some of these cases air-evacuation is the only feasible method of getting the patient to a decompression chamber in time to treat this condition. Flight, however, should be at the lowest possible altitude to avoid aggravating the condition.
Symptom onset timing — DGCA quote
Symptoms and signs usually appear within 15 minutes to 12 hours after surfacing; but in severe cases, symptoms may appear before surfacing or immediately afterwards. Delayed occurrence of symptoms is rare (the source text terminates mid-sentence at the page break — continued in §21+).
Figure 8.5 — Flying after diving: the wait times that keep dissolved nitrogen from bubbling at altitude.
Cross-link recap — the three "wait before flying" rules
You now have three numbers in your head that the DGCA examiner loves to swap around:
Alcohol — bottle to throttle:24 hr (§14.1)
Blood donation:48 hr (§17)
Flying after diving:24 hr (§21)
Flying after rapid decompression:12 hr (§20.4)
Do not mix them up. Diving and alcohol share the 24-hour figure; donation gets the longest pause; rapid decompression "only" 12 — but with mandatory medical clearance afterwards.
§ 22Closing §21 — Delayed DCS After Diving
Picking up the broken sentence
The Part-5 text ended with "Delayed occurrence of symptoms is rare…" — the rest of the sentence (Part 6 source PDF page 22) reads: "…but it does occur, especially if air travel follows diving."
In plain English: even if a diver feels perfectly fine 24+ hours after surfacing, a subsequent flight can re-precipitate DCS symptoms. This is because residual nitrogen still dissolved in slow-perfused tissues (fat, bone marrow) can come out of solution when the pilot enters the lower cabin pressure of a transport flight. The 24-hour rule is a minimum, not a guarantee.